

عنوان الموضوع : تقرير عن الربو باللغة الأنجليزية - الامارات
مقدم من طرف منتديات بيت الامارات النسائي
لو سمحتوا ابا تقرير عن مرض الربو
Please I want a report on asthma
>>>>> ردود الأعضـــــــــــــــــــاء على الموضوع <<<<<
==================================
>>>> الرد الأول :
هلآ ،،
{ .. تقرير عن الربو Asthma .. } ---> بآلعربي ،،
بسم الله الرحمن الرحيم
السلام عليكم ورحمة الله وبركاته
يسرني أن اقدم لكم هذا الملف الطبي والذي يحمل في طياته معلومات متكاملة عن مرض مزمن منتشر والكثير يعاني منه سواء الصغار أو الكبار ألا وهو مرض الربو فتعالوا معنا لنتعرف عليه عن قرب ...
أولا: كيف تعمل الرئتان؟
تعمل شبكة أنابيب الشعيبات الهوائية على إدخال الهواء إلى أنسجة الرئتين وتحمل الهواء المستخدم إلى خارج الجسم. يمر الهواء الداخل من خلال هذه الأنابيب إلى أن يدخل إلى الأكياس الهوائية التي تقع في نهايات أصغر الأنابيب، وهي الموقع الذي يتم فيه تبادل الغاز بين الرئة ونظام الدورة الدموية، حيث يدخل الأكسجين إلى الأكياس الهوائية ويمر منها إلى الأوعية الشعرية ويدخل ثاني أكسيد الكربون من الأوعية الشعرية إلى الأكياس الهوائية ليتم نقله إلى خارج الرئتين.
ثانيا ما هو الربو؟
الربو مرض صدري مزمن تصاب به الرئتين حيث تضيق فيه مجاري الهواء التي تحمل الهواء من وإلى الرئة وبالتالي يصعب التنفس. مجاري الهواء في الشخص المصاب بالربو تكون شديدة الحساسية لعوامل معينة تسمى المهيجات triggers وعند إثارتها بهذه المهيجات تلتهب مجاري الهواء وتنتفخ ويزيد إفرازها للمخاط وتنقبض عضلاتها ويؤدي ذلك إلى إعاقة التدفق العادي للهواء، وهذا ما يسمى بنوبة الربو asthma *ـ*ـ*ـ*ـ*ـ*ـ. بالإمكان السيطرة على أعراض نوبة الربو، ولكن يمكن أن يتكرر حدوث النوبة خلال ساعات بعد حدوث النوبة الأولى. وباختصار هو صعوبة في التنفس تحدث نتيجة لتأثر الرئتين بمواد ( محرضات ) تسبب أزمة الربو . حيث أن الهواء الذي نتنفسه يحمل معه الكثير من الأجسام الدقيقة كغبار الهواء وغبار الطلع . وبينما ينعدم تأثير هذه الأجسام على الشخص العادي إذا استنشقها خلال عملية التنفس ، إلا أن مرضى الربو وبسبب زيادة حساسة الرئتين لديهم فان هذه الأجسام تثير شعبهم الهوائية وتؤدي بالتالي إلى تهيجها وضيقها . تماما كما هو الحال بالنسبة لعينيك عندما تتعرض لدخول الدخان إليها مما يؤدي إلي احمرارها وتهيجها لا يقتصر وجود هذا المرض على منطقة دون أخرى فهناك ما يزيد على 600 مليون شخص مصابين بالربو في مختلف أنحاء العالم لهذا يجب أن لا يشعر مريض الربو بالخجل من مرضه بل عليه أن يعرف كيف يسيطر عليه
ما هي العلامات الأولي المنذرة بحدوث أزمة ربو:
العلامات الأولي هي التغيرات التي تحدث مع بداية حدوث أزمة الربو.
في الحالات الطبيعية، هذه الأعراض لا تكون بالخطورة الكافية التي تجعل المريض يتوقف عن نشاطه الذي يقوم به.إذا شعر المريض بالعلامات الأولي المنذرة لحدوث أزمة قد تساعده في منع حدوث الأزمة أو منع حدوثها بشكل خطير.
- تتضمن هذه العلامات:
- سعال مستمر لا يتوقف، خاصة أثناء الليل.
- ضيق شديد أو بسيط في التنفس.
- الشعور بالإرهاق الشديد أثناء القيام بالرياضة، بالإضافة إلي وجود أزيز في التنفس، سعال وضيق في التنفس.
- نقص أو تغير في سهولة عملية الزفير.
- الشعور بأعراض نزلة البرد – التهاب في الجهاز التنفسي العلوي، الحساسية (العطس، سيلان الأنف، السعال، الاحتقان، تضخم الحلق والصداع).
- أرق.
ما هي نوبة الربو؟
الشخص الذي يصاب بنوبة الربو يجد صعوبة في التنفس، إذ تنقبض العضلات التي تحيط بأنابيب القصبة الهوائية وتؤدي إلى تضييق مجاري الهواء. ويعيق هذا التشنج الشعبي التدفق الطبيعي للهواء، كما تؤدي الزيادة في الإفراز المخاطي إلى تكوين سدادات مخاطية. كذلك يحدث انتفاخ في أنابيب القصبة الهوائية مما يزيد في إعاقة تدفق الهواء. إذا استمرت النوبة فإن استفحال التشنج الشعبي والمخاط يحبس الهواء في الأكياس الهوائية، مما يعيق تبادل الهواء. ويستخدم الشخص الذي يصاب بالنوبة عضلات الصدر بدرجة أكبر لكي تساعده في التنفس.
ما هو الأزيز وكيف يحدث؟
الأزيز صوت يحدث عندما يمر الهواء في مجاري التنفس الضيقة بفعل الانتفاخ والمخاط والتشنج الشعبي. ويمكن أن يحدث الأزيز فجأة ويكون إشارة إلى صعوبة في التنفس. إذا تطورت حدة النوبة قد يختفي الأزيز. إن غياب الأزيز هو إشارة إلى أن الهواء لا يتحرك داخل أو خارج الرئتين، وهذه حالة خطيرة للغاية. سيعود الأزيز مع تحسن النوبة، ويختفي في النهاية تماما.
من يصاب بالربو؟
يمكن لأي شخص أن يصاب بالربو. وهو مرض غير معدي يعاني منه ملايين الناس في كل أرجاء المعمورة بصرف النظر عن العرق أو الثقافة أو السن أو الجنس. ويزيد من احتمال الإصابة بالربو وجود تاريخ عائلي بها. الأشخاص الذين يعانون من الحساسية معرضين أكثر للإصابة بالربو. في الحقيقة يقدر أن 80% من الأطفال و 50% من البالغين المصابين بالربو يوجد لديهم حساسية أيضا. عادة يحدث الربو عند الأطفال في سن الخامسة، وفي البالغين في العقد الثالث، ويمكن أيضا أن يصاب به كبار السن، فحوالي 10% من حالات الربو التي المشخصة تكون بعد سن 65.
* أسباب حدوث أزمة الربو:
ترتبط أزمة الربو بحدوث مشكلة في الممرات الهوائية، لكن السبب الرئيسي لحدوث هذه المشكلة غير معروف.
الممرات الهوائية لدى مريض الربو تكون حساسة للغاية تجاه أي استثارة خارجية وحدوث هذه الاستثارة يسبب حدوث الأزمة.
هناك أنواع مختلفة من الأشياء (الإشارات) التي قد تحدث. ورد فعل الممرات الهوائية تجاه هذه الإشارات تختلف من شخص لآخر ومن وقت لآخر.ومن أهم العوامل الأساسية للتحكم في الربو هي معرفة أسباب حدوث الأزمة ومحاولة تجنبها.
المهيجات الشائعة للربو Triggers
مهيجات الربو هي تلك العوامل التي تعمل على إحداث أعراض الربو، وهذه المهيجات تتفاوت بين المصابين بالربو، ولذلك من الضروري معرفة العوامل التي تحدث النوبة:
العوامل المثيرة للحساسية: ريش أو شعر الحيوانات، عث الغبار (يوجد أيضا في السجاد ومكيفات النوافذ التي لا تنظف دوريا)، غبار الطلع، الأطعمة مثل الفول السوداني والسمك والمحار والبيض.
المثيرات في الهواء:
دخان التبغ من السجائر أو السيجار أو الغليون أو النارجيلة (الشيشة)، دخان الشوي بالفحم، رائحة الطلاء والوقود، الملوثات مثل عوادم السيارات ومداخن المصانع.
الطقس:
الهواء البارد والجاف والرطوبة العالية أو التغيرات المفاجئة بالطقس يمكن أن تسبب أعراض الربو. الرياح تنقل المواد المهيجة المثيرة للحساسية، والمطر يسهل نمو وإطلاق الفطر واللقاح.
المواد المهيجة:
البخاخات (الإيروسول spray/aerosol) والغبار والأبخرة من منتجات التنظيف.
المرض: الالتهابات الفيروسية مثل الزكام/الرشح، الأنفلونزا، التهابات الحلق والجيوب الأنفية تعتبر من المهيجات الشائعة للربو لدى الأطفال.
التمارين الرياضية:
التمارين الرياضية مهيجات شائعة للربو. ويمكن أن تحدث لدى كل الأشخاص المصابين بعد أداء تمارين رياضية عنيفة لمدة 5 دقائق على الأقل. أما الألعاب الرياضية مثل السباحة فهي أقل المهيجات للربو، بينما الجري لمسافات طويلة وكرة القدم عادة ما تؤدي إلى حدوث نوبة الربو عند المعرضين للإصابة.
التغييرات العاطفية:
الضحك والبكاء والخوف والصراخ والسعال يمكن أن تتسبب في أعراض الربو.
-بعض العقاقير مثل: الأسبرين Beta Blockers، العقاقير التي تعالج ارتفاع ضغط الدم، الصداع النصفي والمياه الزرقاء.
تشخيص مرض الربو:
- هناك العديد من الطرق التي يستخدمها الأطباء في تشخيص مرض الربو.
يقوم الطبيب بعمل فحص عام علي المريض، ومعرفة الأعراض التي تحدث له والاطلاع علي التاريخ المرضي.
ثم يقوم بعمل بعض الاختبارات للتعرف علي الحالة الصحية للرئة.
- أشعة "x" الأشعة السينية علي الصدر، وهي صورة للرئة.
- اختبار كفاءة الرئة، وهو اختبار يقوم بقياس كمية الهواء الذي يخرج من الرئة. ويتم ذلك عن طريق النفخ في أنبوب يوضع بين الشفتين، فيتم قياس الزفير الذي يخرج من الرئة.
- اختبار آخر يقوم بقياس سرعة الهواء الذي يخرج من الرئة (الزفير).
- هناك اختبارات أخرى مختلفة مثل اختبارات الحساسية، واختبار الدم.
أهداف علاج الربو
1.التخلص من أعراض الربو ليلا ونهار.
2.التحرر من أي قيد على النشاط اليومي.
3.عدم الاضطرار الى التوجه الى الإسعاف.
4.التخلص من استخدام موسعات الشعب الهوائية بشكل متكرر.
5.الحصول على أفضل قياس لقدرة الهواء.
أدوية الربو
البخاخ أهم طريقة لإعطاء أدوية الربو لأنه يوصل العلاج بشكل مباشر الى الرئتين,
أهم أدوية الصدر:
1 - موسعات الشعب الهوائية (مثل: فنتولين وبريكنيل):
* وتوجد على شكل أقراص وشراب وبخاخ ورذاذ, البخاخ يعتبر أحسن طريقة للاستخدام خصوصا لمن تتجاوز اعمارهم خمس سنوات.
* ينبغي استخدام موسع الشعب الهوائية عند الإحساس بأعراض الربو وليس بشكل مستمر لأن الاستمرار عليه لايؤدي الى زوال الالتهاب المسبب للربو.
2- مشتقات الكورتيزون:
* استخدام مشتقات الكورتيزون عن طريق البخاخ لايؤدي الىحدوث اضرار الكورتيزون المعروفة, ومضار البخاخ محدودة جدا وهي حدوث بحة في الصوت وبعض الالتهابات الفطرية والتي يمكن تجنبها بغسل الفم جيدا بعد البخاخ والغرغرة.
* اقراص الكورتيزون ينبغي قصرها علىالأزمات الحادة في الحالات المتقدمة فقط.
3- هناك الكثير من أدوية الربو مثل:
* أقراص ثيوفلين الموسعة للشعب الهوائية.
* البخاخات الحاوية على مشتقات الكروملين.
* موسعات الشعب الهوائية الحاوية على مادة أتروفنت.
* موسعات الشعب الهوائية طويلة الأمد مثل سيريفنت وأوكسيس.
أنواع البخاخات
البخاخ عبارة عن جهاز يساعد على وصول الجرعة الدوائية الىمجاري التنفس وهناك العديد منها وأكثرها استخداما:
* البخاخات أحادية الجرعة (Metered dose inhalers).
* البخاخ ذو القرص (ديسك هيلر، Diskhaler).
* البخاخ ذو الأقراص (روتواهيلر، Rotahaler).
* البخاخ التربيني عديد الجرعات (تيربو هيلر, Turbohaler) .
.
.
.
__________________________________________________ __________
>>>> الرد الثاني :
{ .. تقرير عن الربو Asthma .. } ---> مترجم للإنجليزي بـgoogle ،،
In the name of God the Merciful
Peace, mercy and blessings of God
I am pleased to offer you the medical file, which carries integrated information for chronic disease is widespread and many suffer from it, whether young or adult asthma, a disease not Come with us to get to know him up close ...
First: How the lungs work?
Pipeline network operating bronchi on the introduction of air into the lungs and tissues of the user to carry air outside the body. Air passes inside through these tubes that enter the air sacs located at the ends of the smallest pipe, a location that is where gas exchange between the lung and circulatory system, which introduces oxygen to the air sacs and passes them to the capillaries and enters the carbon dioxide from the blood poetry to the air bags to be transported out of the lungs.
Secondly, what is asthma?
Asthma is a chronic chest where the lungs become narrow when the ducts that carry air to and from the lung and therefore difficult to breathe. Duct of a person with asthma are very sensitive to certain factors, called triggers triggers and when you raise these irritants become inflamed duct and swell and increase the excretion of mucus and to contract muscles and thereby impeded the normal flow of air, and this is what is called asthma attack asthma ***** *. Possible to control the symptoms of an asthma attack, but can be repeated during a seizure hours after the initial attack. In short, is the difficulty in breathing occurs as a result of the impact on the lungs materials (stimuli) cause asthma. As the air we breathe carries with it a lot of tiny objects air dust and pollen. While no influence of these objects for the average person if inhaled during breathing, but patients with asthma and sensitive lungs because of the increase they have, these objects give rise to air their people and lead to Thejeha and narrow. Just as is the case for your eyes when exposed to the entry of smoke to it, which leads to Ahmrarha and Thejeha not only the existence of this disease on the area without the other there are more than 600 million people with asthma in different parts of the world for that you should not feel sick asthma ashamed of his illness, but it to know how to control it
What are the signs warning of the initial occurrence of asthma:
The first signs are changes that occur with the onset of asthma.
In the normal case, these symptoms are not serious enough to make the patient depends on the activity which he is doing. If a patient feels the initial warning signs of a crisis may help in preventing the crisis or prevent them seriously.
- These Tags:
- Does not stop a persistent cough, especially during the night.
- Very narrow or simple breathing.
- Feeling very tired while doing sports, in addition to the presence of wheezing in breathing, cough and shortness of breath.
- Lack of or change in the ease of the process of exhaling.
- The feeling of cold symptoms - inflammation of the upper respiratory allergies (sneezing, runny nose, cough, congestion, swelling throat, and headache).
- Insomnia.
What is an asthma attack?
The person who gets a heart asthma has difficulty breathing, as to contract the muscles that surround the trachea tubes and lead to narrowing of air ducts. This tension and impede the natural flow of the popular air, as the increase in mucous secretion to the formation of mucous plugs. Occurs as well as swelling of the tracheotomy tubes, thus further impeding the flow of air. If you continue to exacerbate the Nuba People cramping and mucus trap air in the air sacs, which hinders the exchange of air. It uses the person who gets heart chest muscles more in order to assist him in breathing.
What is Pinging and how it happens?
Sizzling sound occurs when air passes in the airways narrow due to swelling and mucus and cramping popular. And wheezing can occur suddenly and be a reference to the difficulty in breathing. If the unit has developed the Nuba wheezing may disappear. The absence of wheezing is a sign that the air does not move inside or outside the lungs, and this situation is very serious. Burr will return with the improvement of the Nuba, and eventually disappear completely.
Who gets asthma?
Anyone can get asthma. It is not contagious disease affecting millions of people all over the world regardless of race, culture or age or sex. And increases the risk of asthma and a family history of it. Persons who suffer from allergies more vulnerable to asthma. In fact, it is estimated that 80% of children and 50% of adults with asthma have as much sensitivity as well. Asthma usually occurs in children in the age of five, and adults in the third decade, and can also be infected by the elderly, about 10% of asthma cases that are diagnosed after the age of 65.
* The causes of asthma:
Associated with asthma of a problem in the airways, but the main reason for the occurrence of this problem is unknown.
Airways of asthma patients are extremely sensitive to any external excitation and the occurrence of such arousal causes a crisis.
There are different types of objects (signals) that may occur. The reaction of the airways to these signals vary from person to person and from time to time. Among the most important key factors to control asthma is to know the causes of the crisis and try to avoid them.
Common triggers for asthma Triggers
Asthma irritants are those factors that bring about symptoms of asthma, this triggers vary among people with asthma, so it is necessary to know the factors that attack occurs:
Factors allergens: feathers or animal hair, dust mites (also found in carpets, windows and conditioners that are not cleaned periodically), pollen, foods such as peanuts, fish, shellfish and eggs.
Stimuli in the air:
Tobacco smoke from cigarettes or cigars or pipe or water pipe (shisha), charcoal grill smoke, the smell of paint, fuel, pollutants such as car exhausts and factory chimneys.
Weather:
Cold, dry air and high humidity or sudden changes of weather can cause asthma symptoms. Wind movement of substances irritating allergens, and rain facilitates the growth and release of mushroom and pollen.
Irritants:
Nebulizer (aerosol spray / aerosol), dust and fumes from cleaning products.
Disease: viral infections such as cold / cold, flu, infections of the throat and sinuses is one of the most common triggers of asthma in children.
Aerobics:
Exercise common irritants for asthma. And can occur in all people with the performance after violent exercise for 5 minutes at least. As for sports such as swimming are less irritants for asthma, while long-distance running and football usually lead to an asthma attack when exposed to infection.
Emotional changes:
Laughter and tears, fear and screaming and coughing can cause asthma symptoms.
- Some drugs, such as: aspirin, Beta Blockers, drugs that treat high blood pressure, migraine and glaucoma.
Diagnosis of asthma:
- There are many ways used by doctors in the diagnosis of asthma.
The work of the doctor examining the patient in, and knowledge of the symptoms that occur to him and look at the history of the patients.
Then doing some tests to find out the health status of the lung.
- Rays "x" x-ray of the chest, an image of the lung.
- Test the efficiency of the lung, which is a test that measures the amount of air that comes out of the lung. This is done by blowing into a tube is placed between the lips, exhaling, which is scaled out of the lungs.
- Another test that measures the speed of the air out of the lungs (exhale).
- There are various other tests such as allergy tests, and a blood test.
The goals of asthma treatment
1. To get rid of the symptoms of asthma at night and day.
2. Free from any restriction on daily activity.
3. Not having to go to the ambulance.
4. Eliminating the use of bronchodilators frequently.
5. To get the best measure of the ability of the air.
Asthma medications
Sprayer most important way to give asthma medication to cure it joins directly to the lungs,
The main medicines Chest:
1 - bronchodilators (eg: Ventolin and Briknyl):
* There are in the form of tablets and syrup and spray and spray, spray is the best way to use especially for those over the age of five years.
* Should be used in an expanded sense of bronchial asthma symptoms and not on an ongoing basis to continue it because of the dysfunctional to the demise of the inflammation that causes asthma.
2 - Cortisone derivatives:
* The use of cortisone derivatives through the spray of dysfunctional Alyhdot damage known as cortisone, and disadvantages of the spray is very limited occurrence of dyspnoea and some fungal infections can be avoided by washing the mouth after a good spray and gargle.
* Cortisone tablets should be limited Alyalozmat acute in advanced cases only.
3 - There are a lot of asthma medications, such as:
* CD Thiovljen bronchodilators.
* Sprays containing derivatives Alkromlin.
* Bronchodilators containing material Otrovnt.
* Bronchodilators such as long-term and Syrevnt Ouksys.
Types of Airbrushes
Sprayer is a device that helps to access Dosage Alymjari breathing and there are many and most commonly used:
* Sprays single dose (Metered dose inhalers).
* Spray a disk (disk Heller, Diskhaler).
* Sprayer with disks (Rotoahilr, Rotahaler).
* Sprayer many doses turbocharger (turbo Heller, Turbohaler).
.
.
.
__________________________________________________ __________
>>>> الرد الثالث :
Asthma is a chronic lung disease in which airways may be inflamed and airway linings become swollen. The airways produce a thick mucus. As the airways narrow, breathing becomes more difficult. The muscles around the airways can also tighten and make the airways narrower. These changes in the airway block the flow of air, making it hard to breathe. This narrowing sometimes gets better by itself, but often requires treatment.
Asthma is unlikely to be a single disease, so we should abolish the term altogether, states an editorial in The Lancet, 27 Aug 2006. People with asthma can have a range of different triggers, symptoms, and responses to treatment, and the general consensus now emerging is that asthma is unlikely to be a single disease entity.
Asthma causes the airways to become very sensitive and to react to contact with many airborne substances. Although it occurs at all ages, it is most common in children under 10. There is a 2:1 male:female ratio in children, which equalizes by the age of 30.
Mild episodic asthma is due primarily to bronchial smooth muscle contraction whereas moderate to severe sustained asthma is largely due to chronic inflammation of the bronchi with the presence of such white cells as eosinophils, neutrophils and mononuclear cells. These cells contribute products that inflame the airways.
People with asthma have airways that are super-sensitive to 'triggers' that do not bother people without asthma. When an asthmatic is near to or comes in contact with a trigger, an asthma episode may start. The airways may become swollen, produce mucus, and tighten up. Common triggers for asthma episodes include the following: Dander (or flakes) of skin, hair, or feathers of all warm-blooded pets
House dust mites
Cockroaches
Pollens from grass and trees
Molds (indoor and outdoor)
Cigarette smoke or wood smoke; scented products such as hair spray, cosmetics, and cleaning products; strong odors from fresh paint or cooking; automobile fumes; and air pollution
Infections in the upper airway, such as colds (a common trigger for both children and adults)
Exercise
Expressing strong feelings (crying, laughing)
Changes in weather and temperature
Some medicines relax the airways while others reduce or prevent the inflammation, swelling and mucus. Severe asthma can be a traumatic, even life-threatening experience. Natural methods of asthma management should be tried prior to or along with conventional treatments.
Please see the link between Asthma and Particulate Avoidance for the importance of having a clean environment.
Although it's not proven, the relatively quick disappearance of H. pylori from our systems is consistent with the idea that widespread antibiotic use is changing human microbiology, which has a consequence, said Dr. Blaser. Other factors in the decline of H. pylori include improvements in childhood living conditions and smaller family size.
"Many studies show that early childhood use of antibiotics is associated with an increased risk of asthma," said Dr. Chen.
In this study, more than one in 10 children under the age of 10 (11 percent) had taken antibiotics in the prior month. Prior studies have shown that by 15, the average child has received three or four courses of antibiotics just for ear infections. "That translates on an annual basis to an extremely high rate of antibiotic use in childhood," she said.
حصلته من هالموقع
https://www.digitalnaturopath.com/cond/C117993.html
__________________________________________________ __________
>>>> الرد الرابع :
أخوي ،، أنآ ترجمت آلتقرير آللي حآطتنه للإنجليزي من قوقل بس مآدري ليش آلمشآركة مب رآضية تستوي ><"
لو تبآ ترجم من google ،، ^.^
و
و
و
آلسموحة // موفقين
__________________________________________________ __________
>>>> الرد الخامس :
Asthma
Asthma is a common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm.[1] Symptoms include wheezing, coughing, chest tightness, and shortness of breath.[2]
Treatment of acute symptoms is usually with an inhaled short-acting beta-2 agonist (such as salbutamol).[3] Symptoms can be prevented by avoiding triggers, such as allergens[4] and irritants, and by inhaling corticosteroids.[5] Leukotriene antagonists are less effective than corticosteroids and thus less preferred.[6]
The prevalence of asthma has increased significantly since the 1970s. As of 2009, 300 million people were affected worldwide.[7] In 2009 asthma caused 250,000 deaths,[7] although generally with treatment, prognosis is good.
Classification
Asthma is clinically classified according to the frequency of symptoms, forced expiratory volume in 1 second (FEV1), and peak expiratory flow rate.[8] Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic), based on whether symptoms are precipitated by allergens (atopic) or not (non-atopic).[9]
While asthma is classified based on severity, at the moment there is no clear method for classifying different subgroups of asthma beyond this system.[10] Within the classifications described above, although the cases of asthma respond to the same treatment differs, thus it is clear that the cases within a classification have significant differences.[10] Finding ways to identify subgroups that respond well to different types of treatments is a current critical goal of asthma research.[10]
Although asthma is a chronic obstructive condition, it is not considered as a part of chronic obstructive pulmonary disease as this term refers specifically to combinations of bronchiectasis, chronic bronchitis, and emphysema. Unlike these diseases, the airway obstruction in asthma is usually reversible; however, if left untreated, asthma can result in chronic inflammation of the lungs and irreversible obstruction.[11] In contrast to emphysema, asthma affects the bronchi, not the alveoli.[12]
-Brittle asthma
Brittle asthma is a term used to describe two types of asthma, distinguishable by recurrent, severe attacks.[13] Type 1 brittle asthma refers to disease with wide peak flow variability, despite intense medication. Type 2 brittle asthma describes background well-controlled asthma, with sudden severe exacerbations.[13]
-Asthma attack
An acute asthma exacerbation is commonly referred to as an asthma attack. The classic symptoms are shortness of breath, wheezing, and chest tightness.[14] While these are the primary symptom of asthma,[15] some people present primarily with coughing, and in severe cases, air motion may be significantly impaired such that no wheezing is heard.[13]
Signs which occur during an asthma attack include the use of accessory muscles of respiration (sternocleidomastoid and scalene muscles of the neck), there may be a paradoxical pulse (a pulse that is weaker during inhalation and stronger during exhalation), and over-inflation of the chest.[16], a blue color of the skin and nails may occur from lack of oxygen.[17]
In a mild exacerbation the peak expiratory flow rate (PEFR) is ≥200 L/min or ≥50% of the predicted best.[18] Moderate is defined as between 80 and 200 L/min or 25% and 50% of the predicted best while severe is defined as ≤ 80 L/min or ≤25% of the predicted best.[18]
-Status asthmaticus
Status asthmaticus is an acute exacerbation of asthma that does not respond to standard treatments of bronchodilators and steroids.
Signs and symptoms
Common symptoms of asthma include wheezing, shortness of breath, chest tightness and coughing. Symptoms are often worse at night or in the early morning, or in response to exercise or cold air.[19] Some people with asthma only rarely experience symptoms, usually in response to triggers, where as other may have marked persistent airflow obstruction.[20]
-Associated comorbidities
-Gastro-esophageal reflux disease
Gastro-esophageal reflux disease coexists with asthma in 80% of people with asthma, with similar symptoms. This is due to increased lung pressures, promoting bronchoconstriction, and through chronic aspiration.[21]
- Sleep Disorders
Due to altered anatomy of the respiratory tract: increased upper airway adipose deposition, altered pharynx skeletal morphology, and extension of the pharyngeal airway; leading to upper airway collapse.[22]
Cause
Asthma is caused by environmental and genetic factors.[23] These factors influence how severe asthma is and how well it responds to medication.[24] The interaction is complex and not fully understood.[25]
-Environmental
Many environmental risk factors have been associated with asthma development and morbidity in children.
Environmental tobacco smoke, especially maternal cigarette smoking, is associated with high risk of asthma prevalence and asthma morbidity, wheeze, and respiratory infections.[26] Low air quality, from traffic pollution or high ozone levels,[27] has been repeatedly associated with increased asthma morbidity and has a suggested association with asthma development that needs further research.[28][29]
Recent studies show a relationship between exposure to air pollutants (e.g. from traffic) and childhood asthma.[30] This research finds that both the occurrence of the disease and exacerbation of childhood asthma are affected by outdoor air pollutants.
Viral respiratory infections are not only one of the leading triggers of an exacerbation but may increase one's risk of developing asthma.[31]
Psychological stress has long been suspected of being an asthma trigger, but only in recent decades has convincing scientific evidence substantiated this hypothesis. Rather than stress directly causing the asthma symptoms, it is thought that stress modulates the immune system to increase the magnitude of the airway inflammatory response to allergens and irritants.[28][32]
Antibiotic use early in life has been linked to development of asthma in several examples; it is thought that antibiotics make children who are predisposed to atopic immune responses susceptible to development of asthma because they modify gut flora, and thus the immune system (as described by the hygiene hypothesis).[33] The hygiene hypothesis (see below) is a hypothesis about the cause of asthma and other allergic disease, and is supported by epidemiologic data for asthma.[34] All of these things may negatively affect exposure to beneficial bacteria and other immune system modulators that are important during development, and thus may cause an increased risk for asthma and allergy.
Caesarean sections have been associated with asthma, possibly because of modifications to the immune system (as described by the hygiene hypothesis).[35]
Respiratory infections such as rhinovirus, Chlamydia pneumoniae and Bordetella pertussis are correlated with asthma exacerbations.[36]
- Genetic
Over 100 genes have been associated with asthma in at least one genetic association study.[37] However, such studies must be repeated to ensure the findings are not due to chance. Through the end of 2005, 25 genes had been associated with asthma in six or more separate populations:[37]
GSTM1
IL10
CTLA-4
SPINK5
LTC4S
LTA
GRPA
NOD1
CC16
GSTP1
STAT6
NOS1
CCL5
TBXA2R
TGFB1
IL4
IL13
CD14
ADRB2 (β-2 adrenergic receptor)
HLA-DRB1
HLA-DQB1
TNF
FCER1B
IL4R
ADAM33
Many of these genes are related to the immune system or to modulating inflammation. However, even among this list of highly replicated genes associated with asthma, the results have not been consistent among all of the populations that have been tested.[37] This indicates that these genes are not associated with asthma under every condition, and that researchers need to do further investigation to figure out the complex interactions that cause asthma. One theory is that asthma is a collection of several diseases, and that genes might have a role in only subsets of asthma.[citation needed] For example, one group of genetic differences (single nucleotide polymorphisms in 17q21) was associated with asthma that develops in childhood.[38]
- Gene–environment interactions
CD14-endotoxin interaction based on CD14 SNP C-159T[39]Endotoxin levelsCC genotypeTT genotypeHigh exposureLow riskHigh riskLow exposureHigh riskLow risk
Research suggests that some genetic variants may only cause asthma when they are combined with specific environmental exposures, and otherwise may not be risk factors for asthma.[23]
The genetic trait, CD14 single nucleotide polymorphism (SNP) C-159T and exposure to endotoxin (a bacterial product) are a well-replicated example of a gene-environment interaction that is associated with asthma. Endotoxin exposure varies from person to person and can come from several environmental sources, including environmental tobacco smoke, dogs, and farms. Researchers have found that risk for asthma changes based on a person’s genotype at CD14 C-159T and level of endotoxin exposure.[39]
- Exacerbation
Some individuals will have stable asthma for weeks or months and then suddenly develop an episode of acute asthma. Different asthmatic individuals react differently to various factors.[40] However, most individuals can develop severe exacerbation of asthma from several triggering agents.[40][41]
Home factors that can lead to exacerbation include dust, house mites, animal dander (especially cat and dog hair), cockroach allergens and molds at any given home.[40] Perfumes are a common cause of acute attacks in females and children. Both virus and bacterial infections of the upper respiratory tract infection can worsen asthma.[40]
Risk factors
Studying the prevalence of asthma and related diseases such as eczema and hay fever have yielded important clues about some key risk factors.[42] The strongest risk factor for developing asthma is a history of atopic disease;[31] this increases one's risk of hay fever by up to 5x and the risk of asthma by 3-4x.[43] In children between the ages of 3-14, a positive skin test for allergies and an increase in immunoglobulin E increases the chance of having asthma.[44] In adults, the more allergens one reacts positively to in a skin test, the higher the odds of having asthma.[45]
Because much allergic asthma is associated with sensitivity to indoor allergens and because Western styles of housing favor greater exposure to indoor allergens, much attention has focused on increased exposure to these allergens in infancy and early childhood as a primary cause of the rise in asthma.[46][47] Primary prevention studies aimed at the aggressive reduction of airborne allergens in a home with infants have shown mixed findings. Strict reduction of dust mite allergens, for example, reduces the risk of allergic sensitization to dust mites, and modestly reduces the risk of developing asthma up until the age of 8 years old.[48][49][50][51] However, studies also showed that the effects of exposure to cat and dog allergens worked in the converse fashion; exposure during the first year of life was found to reduce the risk of allergic sensitization and of developing asthma later in life.[52][53][54]
The inconsistency of this data has inspired research into other facets of Western society and their impact upon the prevalence of asthma. One subject that appears to show a strong correlation is the development of asthma and obesity. In the United Kingdom and United States, the rise in asthma prevalence has echoed an almost epidemic rise in the prevalence of obesity.[55][56][57][58] In Taiwan, symptoms of allergies and airway hyper-reactivity increased in correlation with each 20% increase in body-mass index.[59] Several factors associated with obesity may play a role in the pathogenesis of asthma, including decreased respiratory function due to a buildup of adipose tissue (fat) and the fact that adipose tissue leads to a pro-inflammatory state, which has been associated with non-eosinophilic asthma.[60]
Asthma has been associated with Churg–Strauss syndrome, and individuals with immunologically mediated urticaria may also experience systemic symptoms with generalized urticaria, rhino-conjunctivitis, orolaryngeal and gastrointestinal symptoms, asthma, and, at worst, anaphylaxis.[61] Additionally, adult-onset asthma has been associated with periocular xanthogranulomas.[62]
-Hygiene hypothesis
One theory for the cause of the increase in asthma prevalence worldwide is the so-called "hygiene hypothesis"—that the rise in the prevalence of allergies and asthma is a direct and unintended result of the success of modern hygienic practices in preventing childhood infections.[63] Children living in less hygienic environments (East Germany vs. West Germany,[64] families with many children,[65][66][67] day care environments[68]) tend to have lower incidences of asthma and allergic diseases. This seems to run counter to the logic that viruses are often causative agents in exacerbation of asthma.[69][70][71] Additionally, other studies have shown that viral infections of the lower airway may in some cases induce asthma, as a history of bronchiolitis or croup in early childhood is a predictor of asthma risk in later life.[72] Studies which show that upper respiratory tract infections are protective against asthma risk also tend to show that lower respiratory tract infections conversely tend to increase the risk of asthma.
-Population disparities
Asthma prevalence in the US is higher than in most other countries in the world, but varies drastically between diverse US populations.[28] In the US, asthma prevalence is highest in Puerto Ricans, African Americans, Filipinos, Irish Americans, and Native Hawaiians, and lowest in Mexicans and Koreans.[74][75][76] Mortality rates follow similar trends, and response to Salbutamol is lower in Puerto Ricans than in African Americans or Mexicans.[77][78] As with worldwide asthma disparities, differences in asthma prevalence, mortality, and drug response in the US may be explained by differences in genetic, social and environmental risk factors.
Asthma prevalence also differs between populations of the same ethnicity who are born and live in different places.[79] US-born Mexican populations, for example, have higher asthma rates than non-US born Mexican populations that are living in the US.[80]
There is no correlation between asthma and gender in children, but more adult women are diagnosed with asthma than adult men.[81]
-Socioeconomic factors
The incidence of asthma is highest among low-income populations both nationally[specify] and worldwide. Asthma deaths are most common in low and middle income countries,[82] and in the Western world, it is found in those low-income neighborhoods whose populations consist of large percentages of ethnic minorities.[83] Additionally, asthma has been strongly associated with the presence of cockroaches in living quarters; these insects are more likely to be found in those same neighborhoods.[84]
Most likely due to income and geography, the incidence of and treatment quality for asthma varies among different racial groups.[85] For example, African Americans are less likely to receive outpatient treatment for asthma despite their higher prevalence of the disease. They are much more likely to require an emergency room visit or hospitalization for their asthma symptoms which is probably a contributing factor to their higher likelihood as a race of dying from an asthma attack compared to whites. The prevalence of "severe persistent" asthma is also greater in low-income communities than those with better access to treatment.[85][86]
-Athletics
Asthma appears to be more prevalent in athletes than in the general population. One survey of participants in the 1996 Summer Olympic Games, in Atlanta, Georgia, U.S., showed that 15% had been diagnosed with asthma, and that 10% were on asthma medication.[87]
There appears to be a relatively high incidence of asthma in sports such as cycling, mountain biking, and long-distance running, and a relatively lower incidence in weightlifting and diving. It is unclear how much of these disparities are from the effects of training in the sport.[87][88]
-Occupation
Asthma as a result of (or worsened by) workplace exposures is a commonly reported occupational respiratory disease. Still most cases of occupational asthma are not reported or are not recognized as such. Estimates by the American Thoracic Society (2004) suggest that 15–23% of new-onset asthma cases in adults are work related.[89] In one study monitoring workplace asthma by occupation, the highest percentage of cases occurred among operators, fabricators, and laborers (32.9%), followed by managerial and professional specialists (20.2%), and in technical, sales, and administrative support jobs (19.2%). Most cases were associated with the manufacturing (41.4%) and services (34.2%) industries.[89] Animal proteins, enzymes, flour, natural rubber latex, and certain reactive chemicals are commonly associated with work-related asthma. When recognized, these hazards can be mitigated, dropping the risk of disease.[90]
Diagnosis
There is currently not a precise physiologic, immunologic, or histologic test for diagnosing asthma. The diagnosis is usually made based on the pattern of symptoms (airways obstruction and hyperresponsiveness) and/or response to therapy (partial or complete reversibility) over time.[91]
The British Thoracic Society determines a diagnosis of asthma using a ‘response to therapy’ approach. If the patient responds to treatment, then this is considered to be a confirmation of the diagnosis of asthma. The response measured is the reversibility of airway obstruction after treatment. Airflow in the airways is measured with a peak flow meter or spirometer, and the following diagnostic criteria are used by the British Thoracic Society:[92]
≥20% difference on at least three days in a week for at least two weeks;
≥20% improvement of peak flow following treatment, for example:
10 minutes of inhaled β-agonist (e.g., salbutamol);
six weeks of inhaled corticosteroid (e.g., beclo****sone);
14 days of 30 mg prednisolone.
≥20% decrease in peak flow following exposure to a trigger (e.g., exercise).
In contrast, the US National Asthma Education and Prevention Program (NAEPP) uses a ‘symptom patterns’ approach.[93] Their guidelines for the diagnosis and management of asthma state that a diagnosis of asthma begins by assessing if any of the following list of indicators is present.[93][94] While the indicators are not sufficient to support a diagnosis of asthma, the presence of multiple key indicators increases the probability of a diagnosis of asthma.[93] Spirometry is needed to establish a diagnosis of asthma.[93]
Wheezing—high-pitched whistling sounds when breathing out—especially in children. (Lack of wheezing and a normal chest examination do not exclude asthma.)
history of any of the following:
Cough, worse particularly at night
Recurrent wheeze
Recurrent difficulty in breathing
Recurrent chest tightness
Symptoms occur or worsen in the presence of:
Exercise
Viral infection
Animals with fur or hair
House-dust mites (in mattresses, pillows, upholstered furniture, carpets)
Mold
Smoke (tobacco, wood)
Pollen
Changes in weather
Strong emotional expression (laughing or crying hard)
Airborne chemicals or dusts
Menstrual cycles
Symptoms occur or worsen at night, awakening the patientDifferential diagnosis
The latest guidelines from the U.S. National Asthma Education and Prevention Program (NAEPP) recommend spirometry at the time of initial diagnosis, after treatment is initiated and symptoms are stabilized, whenever control of symptoms deteriorates, and every 1 or 2 years on a regular basis.[95] The NAEPP guidelines do not recommend testing peak expiratory flow as a regular screening method because it is more variable than spirometry. However, testing peak flow at rest (or baseline) and after exercise can be helpful, especially in young patients who may experience only exercise-induced asthma. It may also be useful for daily self-monitoring and for checking the effects of new medications.[95] Peak flow readings can be charted together with a record of symptoms or use peak flow charting software. This allows patients to track their peak flow readings and pass information back to their doctor or nurse.[96]
Differential diagnoses include:[93]
Infants and Children
Upper airway diseases
Allergic rhinitis and sinusitis
Obstructions involving large airways
Foreign body in trachea or bronchus
Vocal cord dysfunction
Vascular rings or laryngeal webs
Laryngotracheomalacia, tracheal stenosis, or bronchostenosis
Enlarged lymph nodes or tumor
Obstructions involving small airways
Viral bronchiolitis or obliterative bronchiolitis
Cystic fibrosis
Bronchopulmonary dysplasia
Heart disease
Other causes
Recurrent cough not due to asthma
Aspiration from swallowing mechanism dysfunction or gastroesophageal reflux
Adults
COPD (e.g., chronic bronchitis or emphysema)
Congestive heart failure
Pulmonary embolism
Mechanical obstruction of the airways (benign and malignant tumors)
Pulmonary infiltration with eosinophilia
Cough secondary to drugs (e.g., angiotensin-converting enzyme (ACE) inhibitors)
Vocal cord dysfunction
Before diagnosing asthma, alternative possibilities should be considered such as the use of known bronchoconstrictors (substances that cause narrowing of the airways, e.g. certain anti-inflammatory agents or beta-blockers). Among elderly people, the presenting symptom may be fatigue, cough, or difficulty breathing, all of which may be erroneously attributed to Chronic obstructive pulmonary disease(COPD), congestive heart failure, or simple aging.[97]Chronic Obstructive Pulmonary Disease
Chronic obstructive pulmonary disease can coexist with asthma and can occur as a complication of chronic asthma. After the age of 65 most people with obstructive airway disease will have asthma and COPD. In this setting, COPD can be differentiated by increased airway neutrophils, abnormally increased wall thickness, and increased smooth muscle in the bronchi. However, this level of investigation is not performed due to COPD and asthma sharing similar principles of management: corticosteroids, long acting beta agonists, and smoking cessation.[98] It closely resembles asthma in symptoms, is correlated with more exposure to cigarette smoke, an older age, less symptom reversibility after bronchodilator administration (as measured by spirometry), and decreased likelihood of family history of atopy.[99][citation needed]Others
The term "atopy" was coined to describe this triad of atopic eczema,allergic rhinitis and asthma.[61]Lifestyle modification
Pulmonary aspiration, whether direct due to dysphagia (swallowing disorder) or indirect (due to acid reflux), can show similar symptoms to asthma. However, with aspiration, fevers might also indicate aspiration pneumonia. Direct aspiration (dysphagia) can be diagnosed by performing a modified barium swallow test. If the aspiration is indirect (from acid reflux), then treatment is directed at this is indicated.[citation needed]
Prevention
The evidence for the effectiveness of measures to prevent the development of asthma is weak.[100] Ones which show some promise include: limiting smoke exposure both in utero and after delivery, breastfeeding, increased exposure to respiratory infection per the hygiene hypothesis (such as in those who attend daycare or are from large families).[100]
Management
A specific, customized plan for proactively monitoring and managing symptoms should be created. Someone who has asthma should understand the importance of reducing exposure to allergens, testing to assess the severity of symptoms, and the usage of medications. The treatment plan should be written down and adjusted according to changes in symptoms.[101]
The most effective treatment for asthma is identifying triggers, such as cigarette smoke, pets, or aspirin, and eliminating exposure to them. If trigger avoidance is insufficient, medical treatment is recommended. Medical treatments used depends on the severity of illness and the frequency of symptoms. Specific medications for asthma are broadly classified in to fast acting and long acting.[102][103]
Bronchodilators are recommended for short-term relief of symptoms. In those with occasional attacks, no other medication is needed. If mild persistent disease is present (more than two attacks a week), low-dose inhaled glucocorticoids or alternatively, an oral leukotriene antagonist or a mast cell stabilizer is recommended. For those who suffer daily attacks, a higher dose of inhaled glucocorticoid is used. In a severe asthma exacerbation, oral glucocorticoids are added to these treatments.[93]
Avoidance of triggers is a key component of improving control and preventing attacks. The most common triggers include: allergens, smoke (tobacco and other), air pollution, non selective beta-blockers, and sulfite-containing foods.[93][104]Medications
Medications used to treat asthma are divided into two general classes: quick-relief medications used to treat acute symptoms; and long-term control medications used to prevent further exacerbation.[105]Other
Fast acting

Salbutamol metered dose inhaler commonly used to treat asthma attacks.
Short acting beta2-adrenoceptor agonists (SABA), such as salbutamol (albuterol USAN) are the first line treatment for asthma symptoms.[3]
Anticholinergic medications, such as ipratropium bromide provide addition benefit when used in combination with SABA in those with moderate or severe symptoms.[3]
Older, less selective adrenergic agonists, such as inhaled epinephrine, have similar efficacy to SABAs.[106] They are however not recommended due to concerns regarding excessive cardiac stimulation.[107]
Long term control

Fluticasone propionate metered dose inhaler commonly used for long term control.
Glucocorticoids are the most effective treatment available for long term control.[108] Inhaled forms are usually used except in the case of severe persistent disease, in which oral steroids may be needed.[108] Inhaled formulations may be used once or twice daily, depending on the severity of symptoms.[109]
Long acting beta-adrenoceptor agonists (LABD) have at least a 12-hour effect. They are however not to be used without a steroid due to an increased risk of severe symptoms.[110][111][112] In December 2008, members of the FDA's drug-safety office recommended withdrawing approval for these medications in children. Discussion is ongoing about their use in adults.[113]
Leukotriene antagonist ( such as zafirlukast) are an alternative to inhaled glucocorticoids, but are not preferred. They may also be used in addition to inhaled glucocorticoids but are second line to LABD.[108]
Mast cell stabilizers (such as cromolyn sodium) are another none preferred alternative to glucocorticoids.[108]
Delivery methods
Medications are typically provided as metered-dose inhalers (MDIs) in combination with an asthma spacer or as a dry powder inhaler. The spacer is a plastic cylinder that mixes the medication with air, making it easier to receive a full dose of the drug. A nebulizer may also be used. Nebulizers and spacers are equally effective in those with mild to moderate symptoms however insufficient evidence is available to determine whether or not a difference exist in those severe symptomatology.[114]
Safety and adverse effects
Long-term use of glucocorticoids carries a significant potential for adverse effects. The incidence of cataracts is increased in people undergoing treatment for asthma with corticosteroids, due to altered regulation of lens epithelial cells.[115] The incidence of osteoporosis is also increased, due to changes inbone remodeling.[116][117]
When an asthma attack is unresponsive to usual medications, other options are available for emergency management.
Oxygen is used to alleviate hypoxia if saturations fall below 92%.[118]
Magnesium sulfate intravenous treatment has been shown to provide a bronchodilating effect when used in addition to other treatment in severe acute asthma attacks.[119][120]
Heliox, a mixture of helium and oxygen, may also be considered in severe unresponsive cases.[120]
Intravenous salbutamol is not supported by available, evidence and is thus used only in extreme cases.[118]
Methylxanthines (such as theophylline) were once widely used, but do not add significantly to the effects of inhaled beta-agonists.[118]
The dissociative anesthetic ketamine is theoretically useful if intubation and mechanical ventilation is needed in people who are approaching respiratory arrest; however, there is no evidence from clinical trials to support this.[121]
Complementary medicine
Many asthma patients, like those who suffer from other chronic disorders, use alternative treatments; surveys show that roughly 50% of asthma patients use some form of unconventional therapy.[122][123] There is little data to support the effectiveness of most of these therapies. Evidence is insufficient to support the usage of Vitamin C.[124] Acupuncture is not recommended for the treatment as there is insufficient evidence to support its use.[125][126] Air ionisers show no evidence that they improve asthma symptoms or benefit lung function; this applied equally to positive and negative ion generators.[127]Increasing frequency
Dust mite control measures, including air filtration, chemicals to kill mites, vacuuming, mattress covers and others methods had no effect on asthma symptoms.[128] However, a review of 30 studies found that "bedding encasement might be an effective asthma treatment under some conditions" (when the patient is highly allergic to dust mite and the intervention reduces the dust mite exposure level from high levels to low levels).[129]
A study of "manual therapies" for asthma, including osteopathic, chiropractic, physiotherapeutic and respiratory therapeutic manoeuvres, found there is insufficient evidence to support or refute their use in treating.[130] The Buteyko breathing technique for controlling hyperventilation may result in a reduction in medications use however does not have any effect on lung function.[131] Thus an expert panel felt that evidence was insufficient to support its use.[125]
Prognosis
The prognosis for asthma is good, especially for children with mild disease.[94][not in citation given] Of asthma diagnosed during childhood, 54% of cases will no longer carry the diagnosis after a decade.[citation needed] The extent of permanent lung damage in people with asthma is unclear. Airway remodeling is observed, but it is unknown whether these represent harmful or beneficial changes.[132] Although conclusions from studies are mixed, most studies show that early treatment with glucocorticoids prevents or ameliorates decline in lung function as measured by several parameters.[133] For those who continue to suffer from mild symptoms, corticosteroids can help most to live their lives with few disabilities. It is more likely to consider immediate medication of inhaled corticosteroids as soon as asthma attacks occur. According to studies conducted, patients with relatively mild asthma who have received inhaled corticosteroids within 12 months of their first asthma symptoms achieved good functional control of asthma after 10 years of individualized therapy as compared to patients who received this medication after 2 years (or more) from their first attacks.[citation needed] Though they (delayed) also had good functional control of asthma, they were observed to exhibited slightly less optimal disease control and more signs of airway inflammation.[citation needed]
Asthma mortality has decreased over the last few decades due to better recognition and improvement in care.[134
Epidemiology
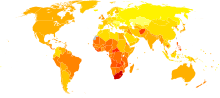
Disability-adjusted life year for asthma per 100,000 inhabitants in 2004.[135] no data <100 100–150 150–200 200–250 250–300 300–350 350–400 400–450 450–500 500–550 550–600 >600

The prevalence of childhood asthma in the United States has increased since 1980, especially in younger children.
As of 2009, 300 million people worldwide were affected by asthma leading to approximately 250,000 deaths per year.[7][110][136][137]
As of 1998, there was a great disparity in prevalence worldwide across the world (as high as a 20 to 60-fold difference), with a trend toward more developed and westernized countries having higher rates of asthma.[138] Westernization however does not explain the entire difference in asthma prevalence between countries, and the disparities may also be affected by differences in genetic, social and environmental risk factors.[28] Mortality however is most common in low to middle income countries,[139] while symptoms were most prevalent (as much as 20%) in the United Kingdom, Australia, New Zealand, and Republic of Ireland; they were lowest (as low as 2–3%) in Eastern Europe, Indonesia, Greece, Uzbekistan, India, and Ethiopia.[138][dated info]
While asthma is more common in affluent countries, it is by no means a restricted problem; the WHO estimate that there are between 15 and 20 million people with asthma in India.[citation needed] In the U.S., urban residents, Hispanics, and African Americans are affected more than the population as a whole.[citation needed] Striking increases in asthma prevalence have been observed in populations migrating from a rural environment to an urban one,[140][dated info] or from a third-world country to Westernized one.[141][dated info]
Asthma affects approximately 7% of the population of the United States[110] and 5% of people in the United Kingdom.[142] Asthma causes 4,000 deaths per year in the United States.[143] In 2005 in the United States asthma affected more than 22 million people including 6 million children.[144] It accounted for nearly 1/2 million hospitalizations,[144] and 14 million missed days of school annually.[citation needed] More boys have asthma than girls, but more women have it than men.[145] Of all children, African Americans and Latinos who live in cities are more at risk for developing asthma.[citation needed] African American children in the U.S. are four times more likely to die of asthma and three times more likely to be hospitalized, compared to their white counterparts.[citation needed] In some Latino neighborhoods, as many as one in three children has been found to have asthma.[146]
In England, an estimated 261,400 people were newly diagnosed with asthma in 2005; 5.7 million people had an asthma diagnosis and were prescribed 32.6 million asthma-related prescriptions.[147]
The frequency of atopic dermatitis, asthma, urticaria and allergic contact dermatitis has been found to be lower in psoriatic patients.[61]
Rates of asthma have increased significantly between the 1960s and 2008.[148][149] Some 9% of US children had asthma in 2001, compared with just 3.6% in 1980. The World Health Organization (WHO) reports that some 10% of the Swiss population suffers from asthma today,[150] compared with just 2% some 25–30 years ago.
History
Asthma was first recognized and named by Hippocrates circa 450 BC. During the 1930s–50s, asthma was considered as being one of the 'holy seven' psychosomatic illnesses. Its aetiology was considered to be psychological, with treatment often based on psychoanalysis and other 'talking cures'.[151] As these psychoanalysts interpreted the asthmatic wheeze as the suppressed cry of the child for its mother, so they considered that the treatment of depression was especially important for individuals with asthma.
from https://en.wikipedia.org/wiki/Asthma
الأخوات ما قصرو
والسموحه تم تغير العنوان ليتناسب مع فحوى الموضوع
بالتوفيق









 رد مع اقتباس
رد مع اقتباس
